
Ongoing Pain and Illness:
Those With a Clear Explanation vs. Those Without
What is Neuroplasticity and What are Neuroplastic Symptoms?
Tens of millions of Americans suffer from ongoing pain or illness. In many cases, people cannot get a clear explanation for their condition even after consulting many different medical professionals. Even when patients do receive a clear explanation and treatment for their chronic symptoms, research shows it is common for them to get little benefit, with pain or illness often persisting for years. Recent evidence points to a potential common cause: neuroplastic symptoms.
This growing area of research shows the brain can generate pain or illness without any associated structural injury or disease, and this can happen across a wide range of symptoms, including back pain, headaches, bowel problems, and more. When pain or illness persists even after injury and disease are ruled out, it is more likely that the symptoms are driven by nerve pathways in the brain (i.e., they are “neuroplastic”). Similarly, in patients whose symptoms are attributed to organ disease or structural injury but who are not responding to treatment as expected, a neuroplastic process is often contributing to their condition. Putting these factors together, we argue that pain or illness is likely to be neuroplastic when a) medical professionals cannot find a clear explanation for the patient’s symptoms, or b) the patient is not responding to treatment as expected.
Recently, we conducted a nationally representative study of US adults to understand how many Americans have a high likelihood of having neuroplastic symptoms, according to the criteria detailed above. We found that nearly half (48%) of Americans have ongoing pain or illness that either has no clear explanation or is not responding to treatment as expected. An overview of the findings are published in our primary report.
How Do People With Explained vs. Unexplained Conditions Differ?
Here, we dive deeper by investigating how opinions and experiences with ongoing pain or illness differ depending on whether people consider their pain or illness to have a clear explanation or not. Specifically, we explore how these two groups of people (those with and without a clear explanation) differ in their symptoms, and whether they are willing to try therapies that focus on addressing stress, trauma, emotions, and other life challenges (i.e., neuroplastic recovery therapies).
For interpreting the data, it is helpful to consider the many variations in how people think about whether their symptoms have a “clear explanation” or “no clear explanation.” For some, they say their pain does not have a clear explanation—perhaps because they have never received a diagnosis or never sought medical advice, or because their symptoms lack a clear structural cause. This often includes symptoms such as headaches and many gastrointestinal symptoms. Even though patients who have been told they have migraine or irritable bowel syndrome may consider this a clear explanation, many will see this as being not clearly diagnosed.
But in many other situations, people may believe they have a clear explanation when in fact their symptoms are neuroplastic. Imagine, for example, a person who strains their back playing tennis and then has persistent pain for years. Initially, their pain was driven by structural damage, but this does not explain pain that persists long after that injury has healed. In these scenarios, the person might believe their pain has a “clear explanation” (the original injury), but not fully recognize the neuroplastic nature of their ongoing pain. In these situations, focusing their treatment on repairing structural damage is in fact a barrier to effective treatment. We can envision many similar stories for symptoms that seem to have more obvious structural roots, such as pain in the muscles, limbs, or joints.
Here, we analyze our national survey data and focus analyses on the part of the population with a high likelihood of having neuroplastic symptoms as defined above (i.e., no clear explanation or the patient is not responding to treatment as expected). Our goal is to deepen understanding of the differences, within this subgroup, between people who say their symptoms have a clear explanation and those who don’t.
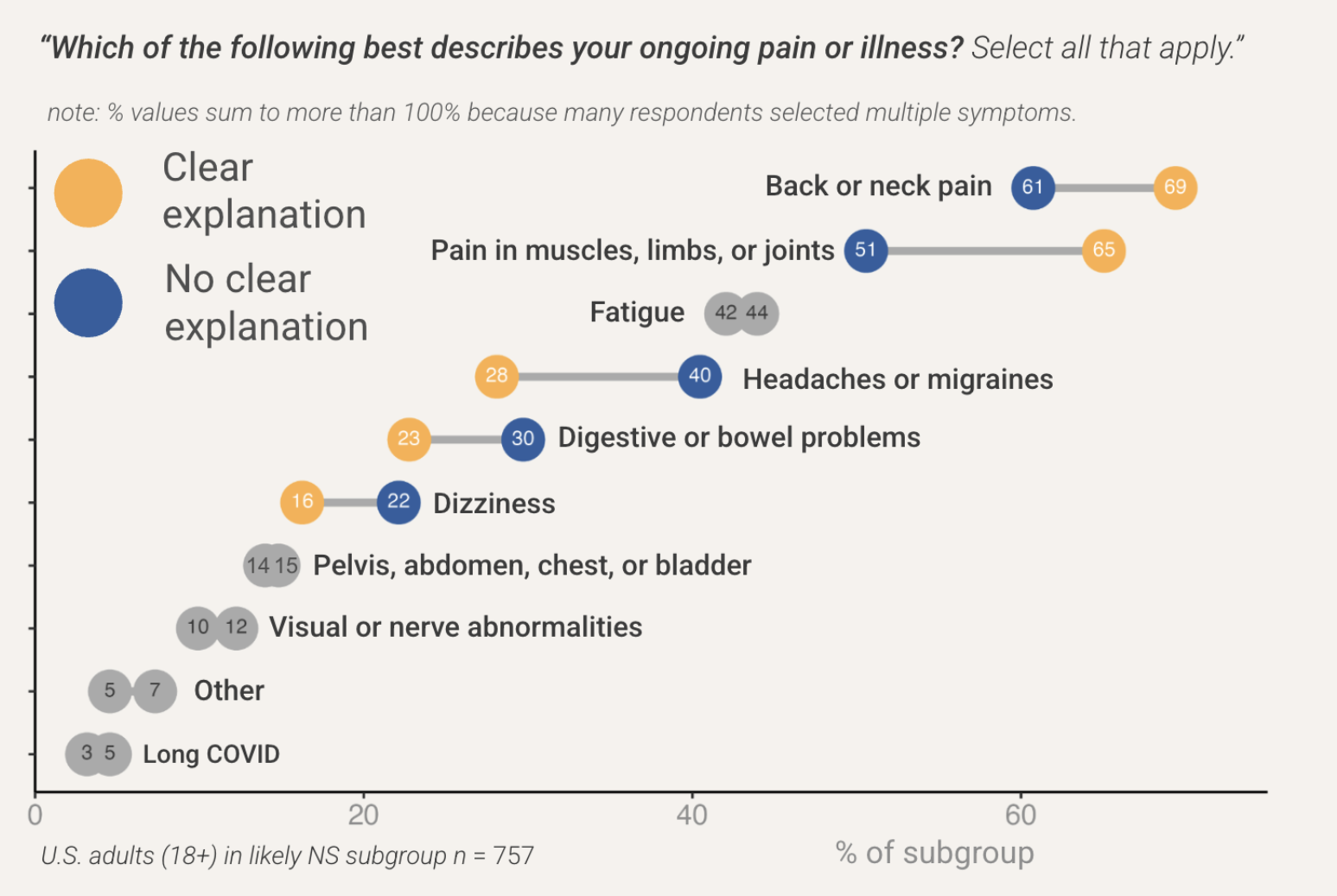
We find some important differences between these groups. As shown in Figure 1, people who say their pain or illness has a clear explanation had a higher prevalence of back or neck pain (+8 pts), and pain in their muscles, limbs, or joints (+14 pts), compared to people with no clear explanation.
We observe the opposite pattern for other symptoms. For people who say their pain or illness does not have a clear explanation, they had a higher prevalence of headaches or migraines (+12 pts), digestive or bowel problems (+7 pts), and dizziness (+6 pts). These findings suggest that certain symptoms are more likely than others to lend themselves to clear explanations––whether or not the explanation correctly identifies the underlying causes.
Figure 1: People are likely to have different symptoms depending on whether they think there is a clear explanation for those symptoms
Another important question to explore is whether having a clear explanation for one’s condition might make people less open to trying neuroplastic treatments. After all, if one believes their pain is caused by structural damage, why try treatments that focus on psychology and the brain?
In our survey, we briefly explained to survey respondents: “Neuroplastic treatment uses education, brain retraining, life insights, and writing exercises to treat ongoing pain or illness,” and then we asked respondents, “How willing or unwilling would you be to try neuroplastic treatments for your own ongoing pain or illness?” Results are shown in Figure 2, separated by those with and without a clear explanation.
Our data show that people who say their pain or illness has a clear explanation report lower willingness to try neuroplastic treatments than people who say they have no clear explanation for their condition. About 39% of people with a clear explanation say they either “definitely” or “probably” would try neuroplastic treatments, whereas 54% of people without a clear explanation say the same. It’s important to note that these group differences are not because they differ in whether they are “unsure” (both 31%), but rather driven by people with a clear explanation being more likely to say they “probably” or “definitely” would not try neuroplastic treatments (27%) compared to people without a clear explanation (13%).
Figure 2: People with no clear explanation for their symptoms are more likely to say they are willing to try neuroplastic treatments

Another open question is how these two groups of people differ in the duration of their symptoms. One plausible hypothesis is that people with a clear explanation would have symptoms for longer because, if symptoms are lasting a long time, the patient seeks out medical advice until an explanation is given. But the opposite pattern is also plausible: people without a clear explanation might have symptoms for longer because it is difficult to treat conditions when the causes are unknown.
Figure 3 shows that, compared to people without a clear explanation, people who say they do have a clear explanation are more likely to have had their symptoms for a longer time. For example, about 26% of people with a clear explanation have had their symptoms for more than 10 years, whereas only 14% of people without a clear explanation have had their symptoms for more than 10 years.
Figure 3: People with a clear explanation for their symptoms tend to have had those symptoms for a longer period of time

It is not clear why these groups differ in the duration of their symptoms, but collectively, these findings are important because they can inform how we approach people with communication efforts. If people’s beliefs about the causes of their symptoms affect their openness to trying new treatments, then we would change the emphasis of our education depending on the audience. For people who believe they have a structural injury, for example, a critical piece of information is how weakly connected imaging results are with experienced pain.
It’s still important to note that, regardless of whether they have a clear explanation, nearly half of people overall with these symptoms say they’d be willing to try neuroplastic treatment, and most others say they are unsure. This means it would be wise to stay focused on building public understanding that these kinds of treatments can be extremely effective for a wide range of symptoms, and many people don’t just reduce their pain or illness–they make a full recovery.
Matthew Goldberg, PhD, and Abel Gustafson, PhD, are Co-founders of XandY—a research and communication strategy firm. David Clarke, MD, is President of the Association for Treatment of Neuroplastic Symptoms.